
Shoulder
Shoulder Replacement
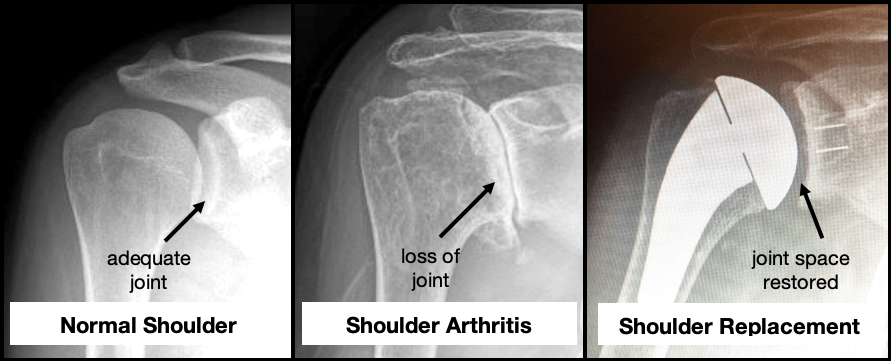
A healthy shoulder joint is lined with cartilage, which acts as a cushion and smooth surface, allowing frictionless movement. Over time, the cartilage can wear down due to osteoarthritis, injury, or other degenerative conditions, leading to pain, stiffness, and difficulty moving the shoulder. If conservative treatments such as medication, physiotherapy, or injections have not been effective, shoulder replacement surgery is often recommended. The goal of the surgery is to relieve pain, restore shoulder mobility, and improve overall function by replacing the damaged joint surfaces with artificial shoulder components.
When is Shoulder Replacement Surgery Needed?
Shoulder replacement surgery is commonly recommended for patients experiencing:
- Severe pain that limits daily activities and mobility
- Bone-on-bone osteoarthritis or degenerative joint disease
- Rotator cuff injuries that cannot be repaired conservatively
- Persistent pain despite non-surgical treatments like physical therapy and cortisone injections
- Difficulty performing overhead activities or reaching out
Procedure for Shoulder Replacement Surgery?
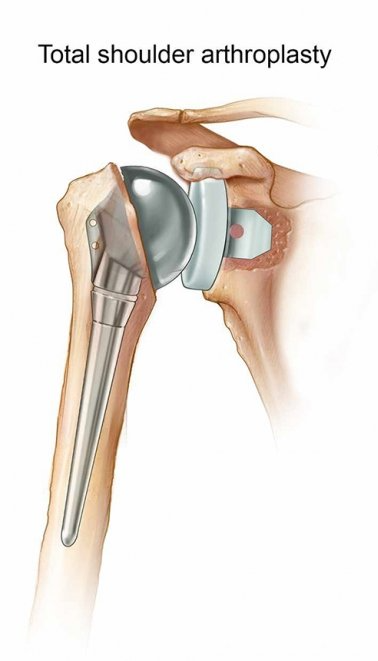
Shoulder replacement, also called total shoulder arthroplasty, involves replacing the humeral head (ball) and the glenoid (socket) with prosthetic components to relieve pain and improve shoulder function.
The surgery is typically indicated when there is bone-on-bone contact in the shoulder joint. During the procedure:
- An incision is made over the shoulder to expose the joint.
- The damaged humeral head is removed, and a humeral stem is placed in the upper arm bone (humerus).
- The glenoid (socket) is cleaned and prepared to accept the glenoid component.
- The components are securely fixed into place, either press-fit or cemented, depending on the patient's bone quality.
The joint capsule is stitched back together, and the muscles and tendons are repaired to ensure optimal alignment.
Benefits of Shoulder Replacement Surgery
- Pain Relief: Significant reduction in shoulder pain, especially for patients suffering from arthritis and degenerative joint disease.
- Improved Range of Motion: Restores shoulder mobility, making it easier to perform everyday activities.
- Long-Term Relief: Effective for patients with bone-on-bone arthritis or severe rotator cuff tears.
Post-Surgery Recovery and Rehabilitation
Pain Management
During the recovery phase, you will be prescribed pain relief medications such as paracetamol and anti-inflammatories. If necessary, stronger pain relievers will be administered in the early stages. Ice packs should be applied for 20 minutes, three to four times a day, to reduce swelling and pain.
Physical Therapy
Physical therapy is a vital component of recovery. The therapy program will focus on:
- Restoring range of motion and improving shoulder strength
- Gradually rebuilding muscle strength and increasing mobility in the shoulder joint
It’s important to follow your physical therapy program to achieve the best possible outcomes.
Return to Work and Sport
Return to Work
Recovery time will vary depending on the nature of your job. After the surgery, you will need to wear a shoulder sling for 2 to 4 weeks. Most people can return to light duties after about two weeks. However, for physically demanding jobs involving lifting, pushing, or overhead activities, you may need up to 12 weeks to resume full duties.
Return to Sport
If you are involved in sports, particularly high-impact or overhead activities, you will need time to recover fully. Most patients can return to non-strenuous activities like cycling or swimming after 4 to 6 weeks, but full recovery for contact sports may take up to 3 to 6 months.
Driving
Patients should avoid driving for 6 weeks or until the sling is removed and shoulder mobility is restored. Dr. du Sart will assess your recovery and provide guidance on when it's safe to drive.
Why Choose Dr. Ryan du Sart for Shoulder Replacement Surgery?
Dr. Ryan du Sart is a highly skilled fellowship-trained orthopaedic surgeon with years of experience in performing shoulder replacement surgeries. His advanced surgical techniques and patient-centered approach ensure that each patient receives tailored care for optimal recovery and pain relief. Dr. du Sart uses state-of-the-art prosthetic components to achieve long-lasting results for his patients.
Book a Consultation with Dr. Ryan du Sart
If you are experiencing shoulder pain, stiffness, or difficulty moving due to arthritis or a rotator cuff injury, shoulder replacement surgery may be the solution. Early intervention can improve your quality of life and restore function to your shoulder.
Contact Dr. du Sart for a consultation to discuss your options for shoulder replacement surgery:
Phone: (08) 9779 9767
Email:
admin@ryandusart.com.au
Clinic Locations:
6 Higgins Street, South Bunbury, WA 6230
20 Prince Street, Busselton, WA 6280
References
- Griffiths, T. (2018). Clinical Outcomes and Benefits of Shoulder Arthroplasty for Cuff Tear Arthropathy. Orthopedic Clinics of North America, 49(1), 123-130.
- Poirier, A., & Martin, S. (2020). Shoulder Replacement Surgery: The Rationale and Results. Journal of Shoulder and Elbow Surgery, 29(5), 917-924.
- Sullivan, D., & McFarland, E. (2019). Innovations in Shoulder Replacement Surgery. Orthopedic Reviews, 11(2), 45-50.
