
Knee
ACL Rupture
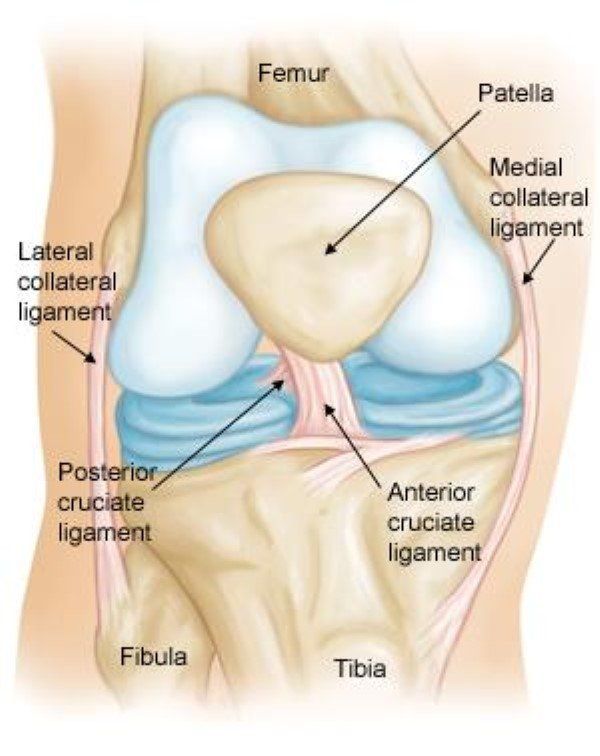
The Anterior Cruciate Ligament (ACL) is one of the four major ligaments in the knee, playing a crucial role in stabilising the knee joint. It runs diagonally through the centre of the knee, connecting the femur (thigh bone) to the tibia (shin bone). The ACL provides essential support during pivoting, twisting, and high-speed movements, preventing the tibia from sliding too far forward over the femur. ACL ruptures are one of the most common knee injuries and can significantly impact a person’s mobility and quality of life.
Causes of ACL Rupture
ACL injuries often occur due to sudden, high-impact movements that stress the ligament beyond its capacity. Common causes of ACL ruptures include:
- Non-contact injuries: Often caused by rapid changes in direction or pivoting during sports activities like basketball, soccer, and skiing.
- Contact injuries: Collisions during sports, such as football or rugby, can result in ACL tears.
- Landing from a jump: Incorrect or awkward landings from a jump can place excessive stress on the knee, leading to ACL tears.
- Rapid deceleration or sudden stops during running or changing direction can also cause ACL injuries.
- According to research, non-contact injuries account for approximately 70% of all ACL ruptures.
Symptoms of ACL Rupture
An ACL rupture is typically very painful, and patients usually report the following:
- Sensation of the knee giving way or buckling during activity
- An audible ‘pop’ sound at the time of injury
- Swelling and pain: The knee will often swell rapidly within hours after the injury
- Inability to bear weight on the affected leg, and difficulty walking
The symptoms can be so severe that they prevent a person from continuing with physical activity, and many experience a lack of trust in the knee’s stability.
Diagnosis of ACL Injury
A thorough physical examination, including a detailed clinical history, is essential for diagnosing an ACL injury. Dr. Ryan du Sart will assess the knee’s range of motion, stability, and ligamentous integrity. The Lachman test and anterior drawer test are commonly used to detect ACL instability. Additionally, MRI imaging is the gold standard for confirming the diagnosis, as it provides a detailed view of the ACL tear and any potential damage to surrounding structures like the menisci, cartilage, and other ligaments .
X-rays may also be used to rule out fractures or bony injuries that could present with similar symptoms.
Treatment Options for ACL Rupture
Treatment for an ACL rupture depends on the severity of the injury, the patient’s age, activity level, and long-term goals. Options include:
Non-Surgical Management
For individuals who are less active, non-surgical treatment may be appropriate. This typically involves:
- Physiotherapy: A tailored physiotherapy program focused on strengthening the muscles around the knee, improving flexibility, and maintaining joint stability.
- Bracing: An ACL brace may be used to stabilise the knee and prevent further injury.
- Activity modification: Avoiding activities that put stress on the knee until rehabilitation is complete.
However, studies have shown that for active individuals, non-surgical management often leads to persistent knee instability and an increased risk of further injury.
Surgical Reconstruction
For patients seeking to return to high-level sports or activities, surgery is often recommended. The ACL does not heal on its own, and the ligament must be reconstructed to restore knee stability. The most common surgical procedure involves replacing the torn ACL with a graft from another tendon in the patient’s body, such as:
- Hamstring tendon
- Patellar tendon
- Quadriceps tendon
The procedure involves carefully removing the damaged ACL and inserting the graft in its place, followed by fixation using screws or other fixation devices. Post-surgical rehabilitation is crucial for ensuring a full recovery and restoring strength to the knee joint.
Find out more about ACL Reconstruction.
Rehabilitation
Post-surgery, rehabilitation is key to restoring function, strength, and stability. The recovery process typically involves:
- Initial Rest and Recovery: Using crutches and a knee brace during the first few weeks after surgery to avoid putting weight on the knee.
- Gradual Physical Therapy: A structured rehab program to rebuild strength and restore range of motion.
- Return to Activity: Patients can usually return to sports or intense physical activities after 6–12 months of rehabilitation, depending on the severity of the injury and the success of the surgery.
Long-Term Risks of Untreated ACL Injuries
If left untreated or inadequately managed, ACL ruptures can lead to significant long-term complications, including:
- Chronic knee instability
- Further ligament damage
- Early-onset osteoarthritis in the knee joint
A study published in The American Journal of Sports Medicine found that patients with untreated ACL injuries are at a significantly higher risk of developing knee osteoarthritis within 10 to 15 years.
Why Choose Dr. Ryan du Sart for Your ACL Injury Treatment
Dr. Ryan du Sart is an experienced orthopaedic surgeon specialising in knee injuries, including ACL ruptures. He provides personalised care to ensure the best possible outcome for his patients, offering both conservative management and advanced surgical options. Dr. du Sart uses the latest technology and evidence-based practices to guide patients through every step of their recovery.
Book a Consultation
If you’re concerned about an ACL injury early intervention is key to better outcomes. Book a consultation with Dr. Ryan du Sart today.
Phone: (08) 9779 9767
Email:
admin@ryandusart.com.au
Clinic Locations:
6 Higgins Street, South Bunbury, WA 6230
20 Prince Street, Busselton, WA 6280
References:
- Hewett TE, et al. "Understanding the mechanism of ACL injuries: Insights from the KNEE". British Journal of Sports Medicine, 2013.
- Webb, J. et al., "ACL Injuries: The Effect of Early Diagnosis on Treatment Outcomes". J Orthop Surg, 2015.
- Sheth, A. et al. "MRI Imaging in ACL Diagnosis and Management". International Orthopaedics, 2017.
- Beynnon, B. D., et al., "ACL Injury Management: Early Surgical versus Non-surgical Intervention". J Bone Joint Surg Am, 2013.
- Kvist, J. et al., "Management of ACL Injuries in Active Adults". Scandinavian Journal of Medicine and Science in Sports, 2014.
- Beynnon, B. D., et al. "ACL Reconstruction: Outcomes and Considerations". Journal of Orthopaedic Research, 2015.
- Pujol, N. et al., "The Role of Physiotherapy Post-ACL Reconstruction". The Knee Journal, 2015.
- Lohmander, S., et al., "Rehabilitation Post-ACL Reconstruction: What’s Best?". Clinical Orthopaedics and Related Research, 2016.
- Myer, G. D., et al., "Long-term consequences of untreated ACL injury: Early-onset osteoarthritis". The American Journal of Sports Medicine, 2017.
