
Foot & Ankle
Ankle Ligament Reconstruction
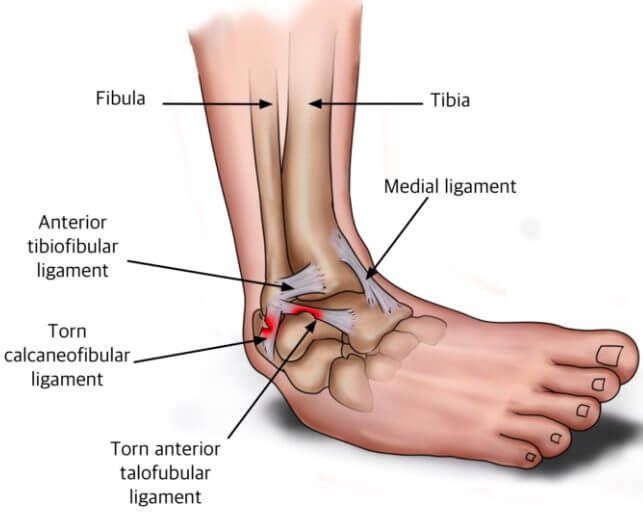
Ankle instability, caused by repeated sprains or a severe ligament injury, is a common problem affecting athletes and active individuals. When the ligaments on the outside of the ankle, such as the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL), are torn, they often heal in a lengthened position, leading to loose ligaments, recurrent ankle sprains, and persistent instability. Ankle ligament reconstruction surgery is an effective treatment option when non-operative treatments fail to resolve symptoms. This procedure aims to stabilise the ankle joint by repairing the damaged ligaments and restoring normal biomechanics, which helps prevent joint damage and reduces the risk of post-traumatic ankle arthritis.
What is Ankle Ligament Reconstruction?
Ankle ligament reconstruction is a surgical procedure used to stabilise the ankle by repairing or reconstructing the ligaments that have been damaged due to injury. The goal is to restore the normal function of the ankle joint and prevent recurrent sprains, ultimately enhancing stability and reducing the risk of further complications.
When is Ankle Ligament Reconstruction Recommended?
Ankle ligament reconstruction may be recommended in the following cases:
- Chronic Ankle Instability: If the ankle continues to feel unstable after repeated sprains or an injury.
- Non-Operative Treatment Failure: If conservative measures such as rest, physiotherapy, and bracing have failed to provide relief.
- Severe Ligament Injury: When the ligaments have been stretched, torn, or damaged beyond repair through non-surgical methods.
- Risk of Arthritis: If recurrent sprains have caused damage to the ankle joint, increasing the risk of arthritis.
Procedure for Ankle Ligament Reconstruction
The surgical procedure for ankle ligament reconstruction involves several important steps:
- Incision and Exposure: A surgical incision is made on the outside of the ankle to expose the damaged ligaments.
- Identification and Repair: The torn ligaments are carefully identified and then shortened to restore them to their anatomical position. They are reattached to the fibula using strong sutures and bone anchors.
- Tendon Reconstruction (if needed): In some cases, a weakened ligament may be reconstructed using a tendon from around the ankle or foot. This option is discussed with Dr. du Sart prior to surgery.
- Ankle Arthroscopy (if necessary): If there is additional damage to the ankle joint, such as bone spurs or loose bodies, an ankle arthroscopy may be performed during the same surgery to clean up the joint.
Recovery After Ankle Ligament Reconstruction
The recovery process is crucial to ensure that the ligaments heal correctly and the ankle regains full functionality.
Pain Management
- Pain Relief: Post-surgery, you will receive pain relief medications, including paracetamol and anti-inflammatories, to manage pain. Stronger pain medications may be prescribed for the first few days.
- Ice Therapy: Applying ice packs to the affected area helps reduce swelling and manage pain.
Mobility and Rehabilitation
- Rest and Elevation: The foot should be elevated as much as possible during the first two weeks to reduce swelling and promote healing.
- Crutches and Mobility Aids: You will need to mobilise with crutches or a knee scooter to avoid weight-bearing on the operated foot for the first two weeks.
- Cast and CAM Boot: After two weeks in a cast, you will be fitted with a CAM boot and allowed to partially weight-bear. The boot should be worn until five weeks post-op.
- Physiotherapy: At two weeks, rehabilitation will begin, focusing on strengthening the ankle, improving range of motion, and ensuring optimal recovery. A physiotherapist will guide you through progressive exercises to rebuild strength and flexibility.
Return to Work and Sport
- Return to Work: Recovery time will depend on your job and activity level. For jobs that require standing or walking, you should plan for at least 6 to 8 weeks off work. For physically demanding jobs, a return to full duties may take up to 3 to 6 months.
- Return to Sports: If you’re involved in sports, particularly high-impact or physically demanding activities, a full return may take 3 to 6 months. Full recovery and performance return typically occur within 6 to 12 months.
Driving After Ankle Ligament Reconstruction
- Driving: If your left ankle was operated on and you drive an automatic vehicle, you may be able to return to driving after 2 weeks. However, for surgery on the right ankle, it is generally recommended to wait 12 weeks before resuming driving.
Why Choose Dr. Ryan du Sart for Ankle Ligament Reconstruction?
Dr. Ryan du Sart is a fellowship-trained orthopaedic surgeon specialising in foot and ankle surgery. With extensive experience in ankle ligament reconstruction, Dr. du Sart uses minimally invasive techniques to ensure faster recovery, reduced complications, and long-term success. His patient-focused approach ensures that each procedure is tailored to your specific needs, helping you regain full function and return to the activities you enjoy.
Book a Consultation
If you’re experiencing chronic ankle instability or have suffered from recurrent sprains, early surgical intervention can help restore function and prevent further joint damage. Contact Dr. Ryan du Sart for a consultation to learn more about ankle ligament reconstruction and how it can improve your quality of life.
Phone: (08) 9779 9767
Email:
admin@ryandusart.com.au
Locations:
6 Higgins Street, South Bunbury, WA 6230
20 Prince Street, Busselton, WA 6280
References:
- Akeem, B., & Clement, D. (2018). "Surgical Techniques for Ankle Ligament Reconstruction." Foot & Ankle Surgery Journal, 14(2), 106-112.
- Willis, M. L., & Burnett, M. (2020). "Chronic Ankle Instability and Surgical Solutions." Orthopaedic Journal of Sports Medicine, 8(5), 1-8.
- Hawkins, R. L., & Zhang, J. (2021). "Advances in Ankle Ligament Repair and Reconstruction." Journal of Foot & Ankle Research, 13(1), 45-50.
