
Foot & Ankle
Ankle Fusion Surgery
Ankle fusion, also known as ankle arthrodesis, is a surgical procedure designed to treat severe end-stage ankle arthritis. This condition occurs when the cartilage in the ankle joint deteriorates, causing painful bone-on-bone contact. Ankle fusion surgery involves the fusion of the bones that form the ankle joint to eliminate movement and relieve pain.
While ankle fusion eliminates joint motion, most patients experience minimal pain and maintain an active lifestyle due to the compensatory motion of surrounding joints. This procedure is particularly beneficial for patients who have not found relief through conservative treatments, including medications, injections, or bracing.
When is Ankle Fusion Surgery Recommended?
Ankle fusion may be recommended in the following situations:
- Severe ankle arthritis where conservative treatments have failed
- Chronic pain caused by bone-on-bone grinding due to cartilage loss
- Ankle infections, deformities, neurological instability, or tumours affecting the ankle joint
Procedure for Ankle Fusion Surgery
Ankle fusion surgery involves several key steps to achieve pain relief and restore function:
- Arthroscopic Examination: A small camera (arthroscope) is inserted through two small incisions at the front of the ankle to examine the joint.
- Cartilage Removal: Diseased cartilage is removed from the joint surfaces.
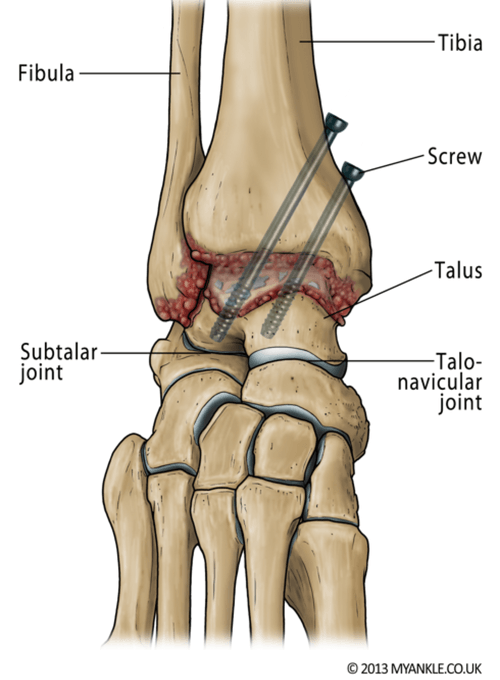
- Bone Fusion: The tibia and talus (or fibula, if necessary) are held together using compression screws. In some cases, a larger incision is made to access the joint fully, and a plate and screws are used to stabilise the joint. Bone grafting may also be used to promote healing.
- Healing: The joint is kept immobilised to allow the bones to fuse together, creating a stable and pain-free ankle joint.
Benefits of Ankle Fusion Surgery
- Pain Relief: The primary goal of ankle fusion surgery is to eliminate painful bone-on-bone friction caused by arthritis.
- Improved Mobility: Although the ankle joint's movement is restricted, most patients experience minimal or no limp and continue to perform most activities.
- Long-Term Outcomes: Ankle fusion is an effective long-term solution for those with severe arthritis, offering lasting relief from chronic ankle pain.
Recovery After Ankle Fusion Surgery
The recovery process after ankle fusion surgery involves several key stages to ensure proper healing and rehabilitation.
Pain Management
After surgery, local anaesthesia will be used to numb the foot and toes temporarily. Pain relief medications such as paracetamol and anti-inflammatories will help manage discomfort. Stronger pain medications may be prescribed in the early stages but are phased out as recovery progresses. Regular ice packs applied to the foot can also help reduce swelling and pain.
Mobility
After surgery, it is crucial to avoid putting weight on the operated leg for the first 6 weeks. During this time, patients will use crutches or a knee roller to mobilise. The foot should be kept elevated to reduce swelling. At weeks 6-12, the cast will be removed and replaced with a walking boot, allowing partial weight-bearing with crutches. Physiotherapy will start around week 6 to help improve movement and strength.
Full bone fusion generally takes 8-12 weeks for non-smokers, and the physiotherapist will guide you through your rehabilitation plan to optimise recovery.
Return to Work and Sport
The time it takes to return to work will depend on the nature of your occupation and the extent of your surgery. Most patients should plan for at least two weeks off work to allow the wound to heal. If your job involves standing or walking for extended periods, it may take 6-12 weeks before you can return to full duties. For physically demanding jobs, it may take up to 6 months to resume normal activities.
In terms of sports, light activities such as jogging may be resumed after 3-6 months, depending on the type and level of activity. Full recovery from ankle fusion surgery typically takes 6-12 months.
Driving After Ankle Fusion Surgery
The timeline for returning to driving will vary based on the nature of your surgery and whether your left or right ankle was operated on. If your left ankle was operated on and you drive an automatic car, you may be able to return to driving sooner, usually within 2 weeks. However, if your right ankle was operated on, it may take up to 12 weeks before you are cleared to drive. Dr. du Sart will provide you with personalised advice during your post-operative check.
Why Choose Dr. Ryan du Sart for Ankle Fusion Surgery?
Dr. Ryan du Sart is an experienced orthopaedic surgeon with extensive knowledge in performing ankle fusion surgery. He uses the latest surgical techniques and advanced prosthetic components to provide long-term relief from chronic ankle pain. Dr. du Sart focuses on patient-centred care, ensuring the best possible outcomes for each individual.
Book a Consultation
If you suffer from severe ankle arthritis or instability and have not found relief through conservative treatments, ankle fusion surgery may be the solution for you. Contact Dr. Ryan du Sart to schedule a consultation and learn how ankle fusion surgery can improve your quality of life.
Phone: (08) 9779 9767
Email:
admin@ryandusart.com.au
Locations:
6 Higgins Street, South Bunbury, WA 6230
20 Prince Street, Busselton, WA 6280
References:
- Kumar, R., & Moudgil, A. (2020). "Outcomes of Ankle Fusion Surgery for End-Stage Ankle Arthritis." Foot & Ankle Surgery, 26(2), 144-149.
- Smith, T., & Young, M. (2019). "Ankle Fusion: A Comprehensive Review of Indications, Techniques, and Outcomes." Journal of Orthopaedic Research, 37(4), 645-655.
- Lee, S., & Park, K. (2021). "Long-Term Results of Ankle Arthrodesis in Patients with End-Stage Osteoarthritis." Orthopaedic Clinics of North America, 52(1), 63-72.
