
Foot & Ankle
Stiff Big Toe (Hallux Rigidus)
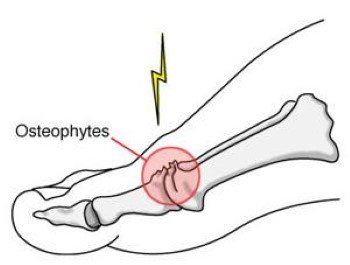
Hallux Rigidus is a degenerative condition affecting the big toe (hallux), specifically the metatarsophalangeal (MTP) joint. This condition is essentially a form of osteoarthritis that leads to pain, stiffness, and reduced movement in the joint. As the cartilage in the joint breaks down over time, it can result in the formation of bone spurs (osteophytes) and other structural changes in the bones. This condition typically causes pain and difficulty in walking, especially during activities that require the toe to bend.
Symptoms of Hallux Rigidus
The symptoms of Hallux Rigidus can vary depending on the severity of the condition. Common symptoms include:
- Pain in the big toe joint during walking or other activities that require toe movement.
- Swelling around the MTP joint, which can worsen with activity.
- A bump or callus on the top of the foot, often with redness around it.
- Stiffness in the big toe, with difficulty bending it, which restricts movement and makes activities such as walking or climbing stairs painful.
Causes of Hallux Rigidus
Hallux Rigidus is typically caused by wear and tear on the big toe joint, which leads to damage of the articular cartilage. Some contributing factors include:
- Injury: A previous traumatic injury or fracture to the big toe can damage the joint cartilage, accelerating the development of arthritis.
- Abnormal foot alignment: Conditions such as flatfoot or bunions can cause excessive pressure on the MTP joint, leading to wear and tear over time.
- Age: Hallux Rigidus is more common in individuals between the ages of 30 and 60 and is associated with the normal aging process of the joints.
- Foot anatomy: Certain types of foot structures or deformities place additional stress on the MTP joint, increasing the risk of developing Hallux Rigidus.
Diagnosis of Hallux Rigidus
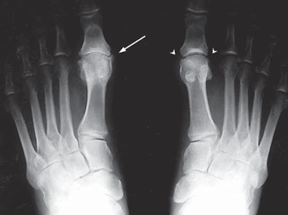
Diagnosis is based on a thorough medical consultation and physical examination. During the examination, your healthcare provider will look for signs of bone spurs, swelling, and limited movement in the big toe. X-rays are used to confirm the diagnosis, showing the extent of cartilage loss, the size of any bone spurs, and the degree of arthritis present in the joint. In some cases, additional imaging such as MRI or CT scans may be recommended to evaluate the joint more comprehensively.
Treatment Options for Hallux Rigidus
Non-Operative Treatment
In the early stages of Hallux Rigidus, treatment typically focuses on managing pain and inflammation while preserving as much joint function as possible. Common non-surgical treatments include:
- Pain management: Medications such as paracetamol or anti-inflammatories (e.g., ibuprofen) may be prescribed to reduce pain and inflammation.
- Footwear changes: Shoes with a wider toe box and rocker-bottom soles can help reduce pressure on the joint, alleviating pain while walking.
- Ice therapy: Applying ice to the joint for 20-30 minutes several times a day can help manage swelling and discomfort.
- Physical therapy: Stretching and strengthening exercises to improve the range of motion and reduce stiffness.
- Orthotics: Custom-made insoles or arch supports to redistribute pressure away from the joint and improve function.
- Contrast baths: Alternating between hot and cold water soaks to promote circulation and relieve pain.
Surgical Treatment
If non-operative treatments are unsuccessful and the condition progresses, surgery may be recommended. Surgical options vary based on the severity of the condition and include:
- Cheilectomy: This surgery is recommended for patients with mild to moderate Hallux Rigidus. It involves the removal of bone spurs and part of the affected bone to allow for better joint movement. This procedure is minimally invasive and typically requires no postoperative immobilization. (Kay, 2017). Find out more about Cheilectomy.
- Arthrodesis (Fusion): In cases of severe arthritis, where the cartilage is extensively damaged, a joint fusion may be recommended. This procedure involves removing the damaged cartilage and using screws or plates to fuse the bones together, eliminating pain but also eliminating movement in the joint. While patients experience pain relief, they may lose some degree of foot mobility. (Smith et al., 2018). Find out more about Ankle Fusion.
- Arthroplasty (Joint Replacement): In rare cases, particularly for
older patients with low functional demands, a joint replacement may be an option. The damaged joint surfaces are replaced with an artificial implant made of metal and plastic. While this procedure has had mixed results, advancements in materials are improving its long-term success. (Lee & Choi, 2020). Find out more about
Ankle Replacement.

Why Choose Dr. Ryan du Sart for Hallux Rigidus Treatment?
Dr. Ryan du Sart is a highly trained orthopaedic surgeon with extensive experience in diagnosing and treating Hallux Rigidus and other foot and ankle conditions. He offers a personalised, patient-centred approach to treatment, tailoring care plans to each patient’s unique needs, from conservative therapies to advanced surgical interventions.
Book a Consultation
If you are experiencing foot pain or stiffness in the big toe, early diagnosis and treatment can help prevent further joint damage. Schedule a consultation with Dr. Ryan du Sart today to discuss your treatment options and get on the path to recovery.
Phone: (08) 9779 9767
Email: admin@ryandusart.com.au
Locations:
6 Higgins Street, South Bunbury, WA 6230
20 Prince Street, Busselton, WA 6280
References:
- Kay, D. (2017). "Cheilectomy for Hallux Rigidus: A Review of Outcomes." Journal of Foot and Ankle Surgery, 56(4), 767-774.
- Smith, S. L., et al. (2018). "Arthrodesis versus Cheilectomy in Severe Hallux Rigidus: A Long-Term Outcome Study." Foot and Ankle International, 39(7), 805-811.
- Lee, D. J., & Choi, J. W. (2020). "The Role of Total Joint Replacement in Hallux Rigidus Treatment." Orthopaedic Clinics of North America, 51(2), 249-258.
