
Knee
ACL Reconstruction
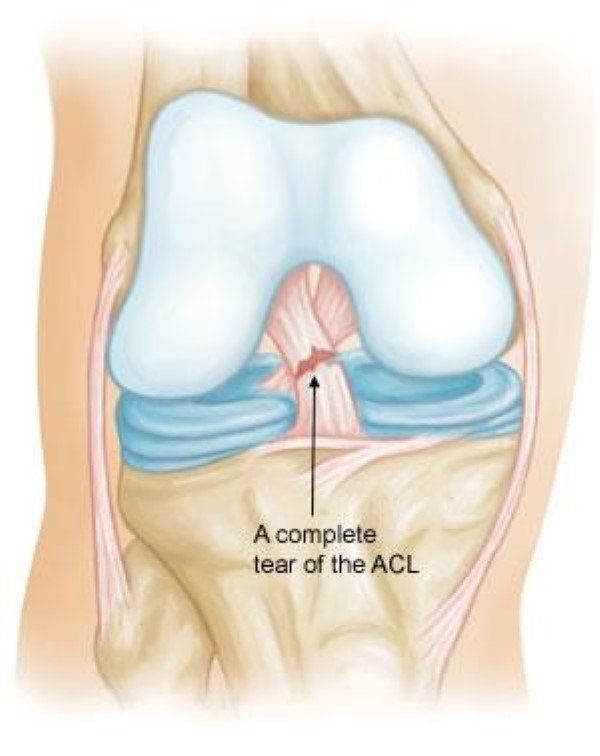
An Anterior Cruciate Ligament (ACL) rupture is a common and often debilitating knee injury, particularly for athletes. ACL injuries typically occur due to sudden twists, pivoting movements, or direct impacts. Left untreated, ACL tears can lead to long-term instability, difficulty in bearing weight, and a higher risk of further damage to the knee joint. Fortunately, ACL reconstruction surgery provides a highly effective solution to restore stability and function, allowing patients to return to their daily activities, including sports.
What is ACL Reconstruction?
ACL reconstruction surgery is performed to replace a torn anterior cruciate ligament (ACL)
with a tendon graft. This surgery is commonly recommended when non-surgical treatments fail to provide adequate results or if the patient experiences significant instability. Unlike some knee procedures, ACL reconstruction is typically performed arthroscopically (minimally invasive surgery), which offers several advantages, including smaller incisions, less post-operative pain, and faster recovery.
Procedure: What to Expect
ACL reconstruction surgery involves the removal of the damaged ligament and the insertion of a graft tendon to replace it. The graft can be taken from your own body (autograft), a donor (allograft), or synthetic sources (such as LARS). The surgery is performed through small incisions around the knee, which limits scarring and speeds up recovery.
The surgical process generally includes:
- Removal of the damaged ACL: The old ligament is removed, and small holes are drilled into the femur and tibia to allow for the placement of the new graft.
- Insertion of the graft: The graft is passed through the bone tunnels, and it is secured using screws or other devices, ensuring the ligament heals in place.
- Other procedures: If additional knee damage, such as meniscus tears, is present, it may be treated during the same procedure.
The surgery typically takes about 1-2 hours to complete, and most patients are discharged after an overnight stay.

Recovery After ACL Reconstruction Surgery
Recovery after ACL reconstruction is a critical process that requires dedication to rehabilitation. The success of the surgery heavily relies on post-operative care, especially in the early stages.
Stage 1: Acute Phase (0 to 2 Weeks)
Goals:
- Promote wound healing and manage pain
- Reduce swelling
- Restore range of motion (near full extension)
- Begin to establish muscle control around the knee
During this phase, patients are advised to rest, ice, elevate the knee, and follow the R.I.C.E. (Rest, Ice, Compression, Elevation) method. Crutches may be used for the first few weeks, and full extension of the knee should be achieved without hyperextension to avoid stretching the graft.
Stage 2: Early Rehabilitation (2 to 6 Weeks)
Goals:
- Achieve full range of motion (extension and flexion)
- Restore normal walking patterns
- Improve muscle control and strength
During this period, patients should continue to reduce swelling, perform gentle exercises to restore knee mobility, and increase weight-bearing activity gradually.
Stage 3: Strengthening (6 to 12 Weeks)
Goals:
- Increase quadriceps strength
- Improve balance and proprioception
- Progress to light running and gradual change of direction
Patients will begin strengthening exercises, such as using a stationary bike or light swimming. Strengthening the quadriceps and hamstrings is vital to support the knee joint during dynamic movements.
Stage 4: Sport-Specific Training (3 to 6 Months)
Goals:
- Improve muscle strength and endurance
- Perform sport-specific drills
- Build running endurance, jumping, and change of direction skills
This stage involves sport-specific drills and more aggressive exercises, including running and agility work, with the goal of returning to active sports.
Stage 5: Full Return to Sport (6 to 12 Months)
Goals:
- Gradual reintroduction to sport-specific skills
- Full training for competitive activities
- Prepare for game simulation to ensure readiness for sport
By 9 to 12 months post-surgery, most patients can return to sports, particularly those that involve pivoting and high-intensity movements. Return to contact sports will depend on the individual’s recovery and strength.
Return to Work and Activity
The return to work after ACL surgery depends on the type of work you do. For most patients, taking 2-4 weeks off work is necessary to allow initial healing. Labour-intensive work may require 6-12 weeks before a safe return. Physical therapy continues throughout this period, and high-impact activities, such as running or jumping, should be avoided for at least 12 weeks.
Driving After ACL Surgery
The timing for returning to driving depends on the knee operated and the individual’s recovery. For patients with left knee surgery and an automatic car, driving may resume after 3 to 4 days, whereas patients with right knee surgery may need 4-6 weeks before driving. Dr. du Sart will advise when it is safe to return to driving.
Why Choose Dr. Ryan du Sart for ACL Reconstruction?
Dr. Ryan du Sart is an experienced orthopaedic surgeon specialising in ACL reconstruction surgery. He has extensive expertise in both traditional and robotic-assisted techniques, providing individualised treatment plans to ensure the best outcome. Using the latest minimally invasive surgical techniques, Dr. du Sart aims to restore knee stability and function, allowing patients to return to a pain-free and active lifestyle.
Book a Consultation
If you’ve suffered an ACL rupture or are experiencing knee instability, early diagnosis and ACL reconstruction surgery may be the best solution for you. Book a consultation with Dr. Ryan du Sart today to discuss your treatment options and begin your journey to recovery.
Phone: (08) 9779 9767
Email:
admin@ryandusart.com.au
Clinic Locations:
6 Higgins Street, South Bunbury, WA 6230
20 Prince Street, Busselton, WA 6280
References:
- Baker, P., et al. (2012). "ACL Injury and Reconstruction: A Review of Current Approaches and Clinical Outcomes." Orthopaedic Journal of Sports Medicine.
- Australian Orthopaedic Association (AOA). "National Joint Replacement Registry." Annual Report, 2022.
- Webster, K., & Feller, J. (2020). "Outcomes of ACL Reconstruction: A Systematic Review." The American Journal of Sports Medicine.
