
Foot & Ankle
Cheilectomy
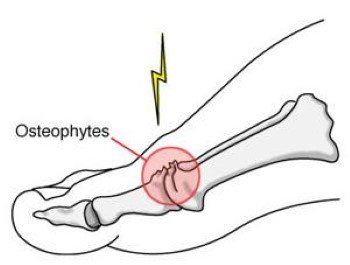
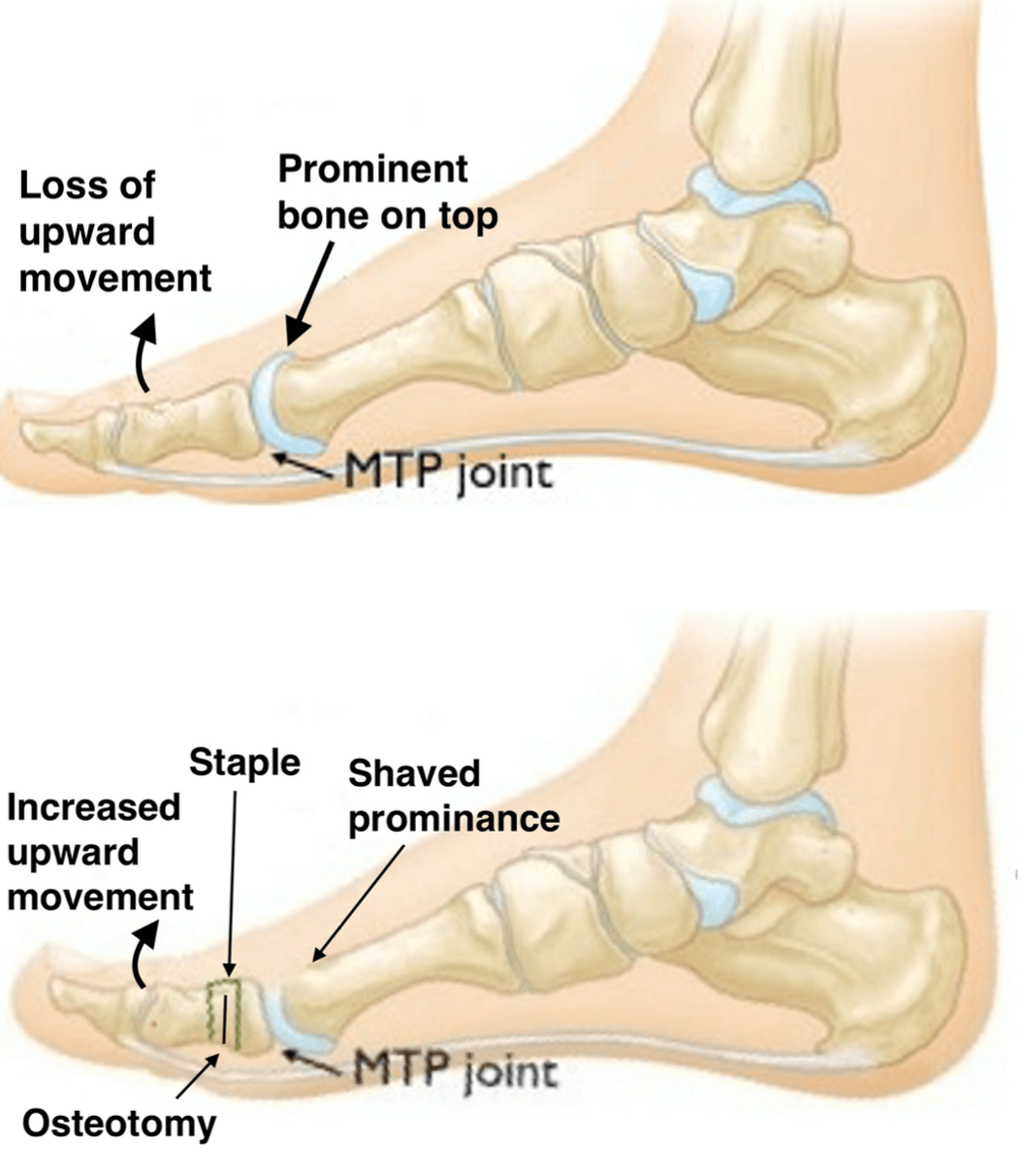
Cheilectomy is a surgical procedure commonly recommended for patients suffering from Hallux Rigidus, a degenerative condition of the big toe joint (metatarsophalangeal or MTP joint). Hallux Rigidus causes pain, stiffness, and limited movement due to the loss of cartilage, the formation of bone spurs (osteophytes), and changes in the bone structure (sclerosis). This condition restricts the toe's mobility and causes pain when walking. Cheilectomy is a minimally invasive procedure aimed at relieving pain and restoring function by removing bone spurs and any bone buildup that interferes with joint movement.
When is Cheilectomy Recommended?
Cheilectomy is typically recommended for individuals with mild to moderate Hallux Rigidus who experience the following:
- Pain and stiffness in the big toe joint
- Difficulty moving the toe
- Bone spurs (osteophytes) and cartilage degeneration in the joint
- Difficulty with activities such as walking, running, or standing for long periods
In some cases, if the disease progresses, the patient may require further procedures, such as arthrodesis (joint fusion) or arthroplasty (joint replacement).
Procedure for Cheilectomy
Dr. Ryan du Sart performs minimally invasive (keyhole) cheilectomy for most patients. This approach offers several benefits, including smaller incisions, less soft tissue damage, reduced pain and swelling, and a faster recovery. The procedure involves the following steps:
- Incision and Exposure: A small incision is made on the top of the big toe to access the joint.
- Removal of Bone Spurs: Excess bone and any bony buildup around the joint that restricts normal movement are removed to allow the toe to move freely.
- Joint Alignment (if necessary): In rare cases, the joint may need to be realigned. This is done with X-ray guidance and may require screws for stabilisation of the alignment.
- Closure: After the procedure, the incision is closed, and a sterile dressing is applied.
Benefits of Cheilectomy
- Pain Relief: The procedure effectively alleviates the pain caused by Hallux Rigidus, providing long-term relief for many patients.
- Improved Mobility: By removing the bone spurs and any obstructions in the joint, the toe can move more freely, restoring function and reducing stiffness.
- Minimally Invasive: The keyhole surgery approach ensures less scarring and a faster recovery compared to traditional open surgery.
Recovery After Cheilectomy
Recovery from cheilectomy involves several stages, with a focus on pain management, mobility, and rehabilitation to restore full function of the toe:
Pain Management
- After surgery, the foot is elevated to reduce swelling, and local anaesthesia will provide pain relief and numb the foot temporarily.
- Regular pain relief medications such as paracetamol and anti-inflammatories are typically prescribed, with stronger medications used in the initial stages and phased out as comfort improves.
- Applying ice packs to the foot can help alleviate pain and reduce swelling.
Mobility
- Initially, you will be able to walk with a surgical shoe for support, and crutches may be used if necessary.
- It is important to keep the foot elevated for the first few days to manage swelling and discomfort.
- After approximately two weeks, you will continue walking with the surgical shoe, and gradually transition to wider shoes to improve comfort.
- A tailored rehabilitation program will be provided to help reduce muscle tightness and improve mobility. This will include stretches and exercises to promote proper movement and strength in the foot.
Return to Work and Sport
- Return to Work: Recovery time will vary depending on the nature of your work. You should plan for at least two weeks off work to allow the wound adequate time to heal and elevate your leg. For light duties, you may return after two weeks. However, if your job requires you to be on your feet or engage in physical activity, it may take 4 to 6 weeks before you're able to resume full duties.
- Return to Sports: The time required to return to jogging and other sports will depend on your activity level and the type of surgery performed. Generally, returning to sports may take 3 to 6 months, with full recovery expected in 6 to 12 months.
Driving After Surgery
- If your left foot was operated on, you may return to driving after two weeks, assuming you feel comfortable.
- If the right foot was operated on, you are advised to wait 3 weeks before returning to driving, but this may vary based on your individual recovery and ability to control the vehicle safely.
- Discuss any concerns regarding driving with Dr. du Sart during your post-op check.
Why Choose Dr. Ryan du Sart for Cheilectomy?
Dr. Ryan du Sart is an experienced orthopaedic surgeon with extensive expertise in performing cheilectomy procedures. He uses state-of-the-art techniques and provides personalised care to ensure the best outcomes for his patients. His patient-centred approach ensures each individual receives the most effective and tailored care for optimal recovery.
Book a Consultation
If you are experiencing pain or stiffness in the big toe due to Hallux Rigidus and have been considering a cheilectomy, contact Dr. Ryan du Sart for a consultation. He can help determine whether this procedure is right for you and provide solutions to relieve your pain and improve your quality of life.
Phone: (08) 9779 9767
Email:
admin@ryandusart.com.au
Locations:
6 Higgins Street, South Bunbury, WA 6230
20 Prince Street, Busselton, WA 6280
References:
- Goff, M., & Gellman, R. (2018). "Outcomes of Cheilectomy for Hallux Rigidus: A Systematic Review." Journal of Foot and Ankle Surgery, 57(3), 515-522.
- Yeo, S., & Tan, K. (2020). "Surgical Techniques and Results of Cheilectomy for Hallux Rigidus." Foot & Ankle International, 41(4), 460-467.
- Malerba, G., & Smith, R. (2019). "Cheilectomy vs. Arthrodesis: A Comparative Study of Hallux Rigidus Treatment." Orthopaedic Reviews, 11(2), 35-42.
